Pulsara goes to the World Cup: Supporting Medical Response with Connected Communication
With record-breaking crowds filling stadiums across North America, the 2026 FIFA World Cup is proving to be one of the largest sporting events in...

Prior to the COVID-19 pandemic, Teller County, Colorado, had a successful community paramedicine program in place. But as the pandemic hit the U.S., they knew they'd need to leverage new tools to continue treating their patients. Fire and EMS leaders partnered with Pulsara to enhance their community paramedicine program with telehealth. Since then, the program has evolved into a thriving partnership between EMS and a local organization of board-certified emergency physicians, allowing them to work together via telehealth to help address healthcare disparities and improve access to care in rural areas.
In a recent webinar, EMS leadership in Teller County, Colorado, shared their experiences around building the program, and how they are using telehealth as a force multiplier to preserve resources while also better meeting the needs of their community. Here are 7 top takeaways from their experience.
Historically, telehealth has not been associated with fire or EMS. Traditional telehealth appointments involve a scheduled phone or video call between a patient and a physician. However, during the COVID-19 pandemic, all clinicians needed ways to continue connecting with patients without always being present with them in person. The concept of using telehealth to enhance calls for fire and EMS gained steam.
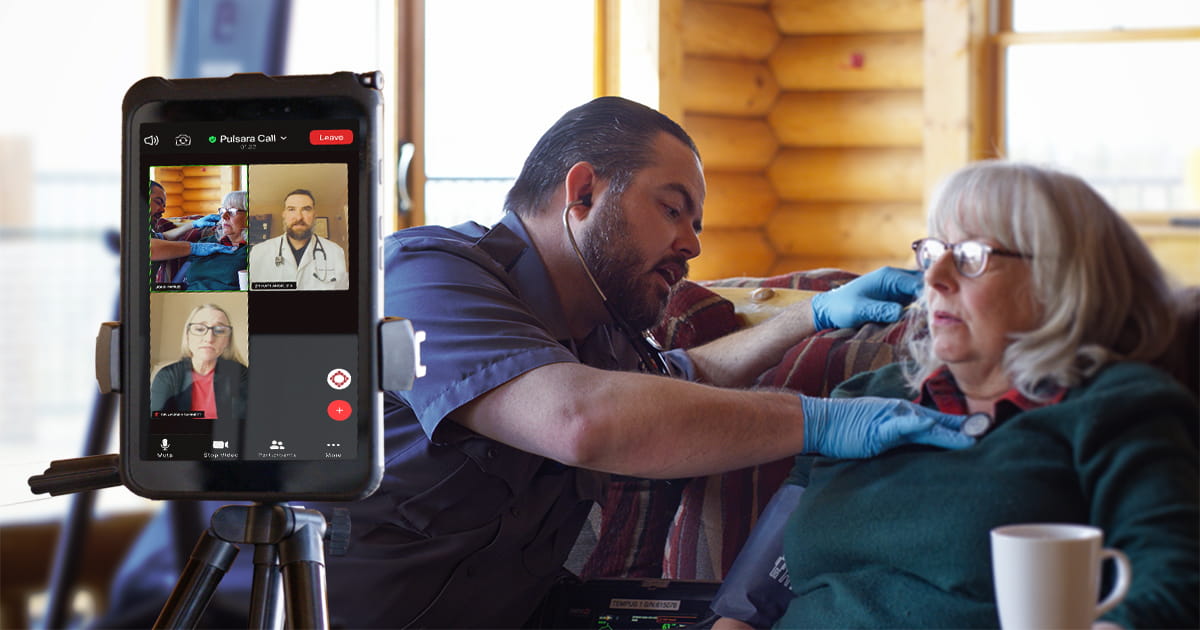
While it’s a handy way to help care for patients when an in-person visit isn’t possible, video has its limitations. James McLaughlin, Director of Community Paramedicine at Ute Pass Regional Health Service District, explained: “Providing care in a telehealth platform is limiting. You don't have any peripheral vision. …You don't get to hear the patient's heart tones, you don't get to hear their lung sounds. You don't get to touch the patient and actually feel that they're hot to the touch.”
McLaughlin joined forces with Dr. Jeremy DeWall, EMS Medical Director at UCHealth Pike's Peak Regional Hospital, to devise a solution. They paired telehealth with a modernized form of how medical care was delivered for thousands of years: the traditional house call.
“We all remember those old TV shows, or if you’ve read old books—Little House on the Prairie, and things like that,” said McLaughlin. “The doctor used to show up, and you paid him an apple pie. Obviously, a system like that doesn't work anymore, but it doesn't mean that you can't increase a patient's access to a board-certified physician. That's what we work to do with this program. We want to bring that provider into your home in a meaningful way while still being respectful of their time so that they are able to be available for a lot of other patients.”
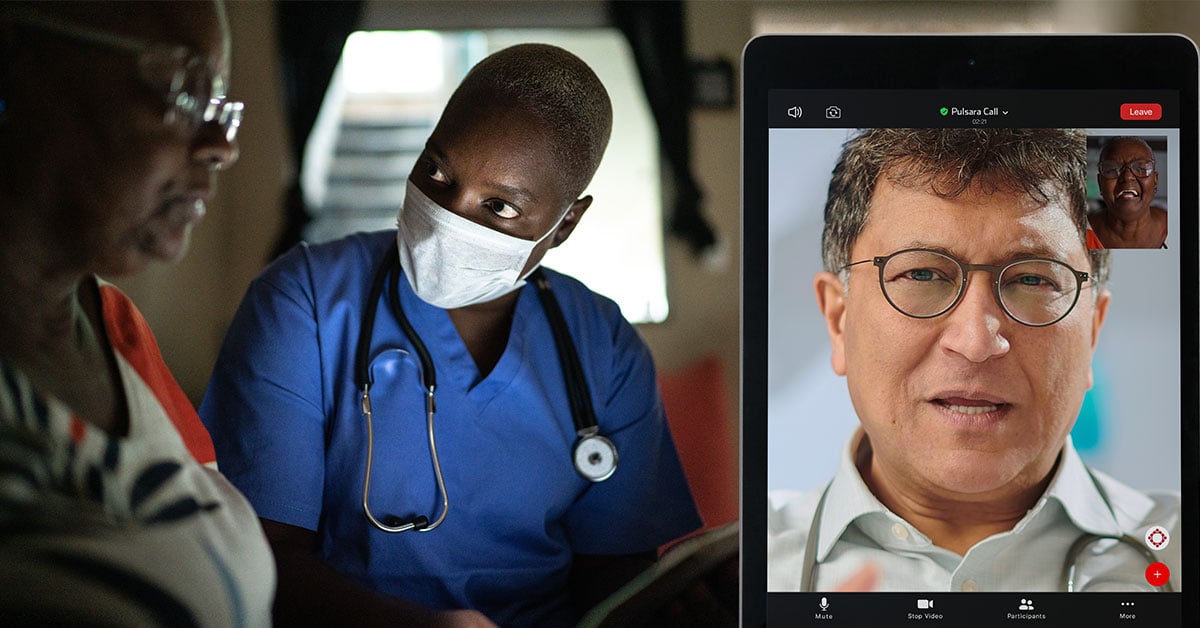
While the physician can’t travel to be onsite with the patient, the community paramedic can, and they can act as the physician’s eyes and ears. The paramedic examines the patient in person and can communicate to the doctor what they’re seeing, giving the physician a more complete idea of the patient’s condition. “The community paramedic adds that peripheral vision,” said McLaughlin. “They actually get to see the entire environment that the patient is living in and can help identify challenges.”
According to McLaughlin, this form of telehealth is not only more reassuring to patients than traditional telehealth—it’s also safer. “It gives the physician more to work with and provides them with a much larger picture so that they can engage with that patient in a safer and more meaningful way. We add an extra level of safety to the process and an extra level of value for the patient.”
Before starting the program, Ute Pass Regional Health Service District (UPRHSD) was facing increased need for their services, but no additional resources to help meet the need. “With our call volume at the inception of this program, we probably needed five ambulances if we were going to use a traditional model, [which was to] transport everybody to the hospital,” said McLaughlin.
As a result, they began looking at telehealth in a new light. What if it could help maximize their current resources by keeping ambulances available, while still delivering high-quality care for patients—in most cases, even better and more personalized service than they would have otherwise received?
By dispatching community paramedics in other vehicles, UPRHSD kept ambulances free while offering their patients a chance to be examined by an experienced community paramedic and to speak directly with a board-certified emergency physician—from the comfort of their own home. “This model allows us to do more with less,” McLaughlin explained. “We still have our three ambulances, and they're available. But now the community paramedic can go out as a single resource, do evaluations, provide assessments, do care, and keep that patient where they really want to be—at home—and get them the services that they need and get them connected with the ongoing care. My ambulances are still in service and still available for those life-threatening emergency calls for those patients that absolutely do need to go to the emergency room. A force multiplier is just that: It's a way to take your existing workforce and multiply what it's able to do and add value to your community.”
In rural and frontier areas, reaching and transporting a single patient to the hospital can take a long time—sometimes up to several hours. Dr. DeWall explained how telehealth shortens the time to getting a patient care: “In some of our areas, especially in rural areas where we have transport times of an hour and a half to the hospital and a return time to the service area of relatively similar, we can do a telehealth call and be in and out of that patient's home in 20 minutes, sometimes less, sometimes a little more, compared to a three-hour time-on-task transporting a patient to a hospital.”
While the approach takes longer than doing a release-of-care, it’s ultimately a much more satisfying experience for both the patient and the provider. It also saves time by getting patients the right care the first time, preventing the need for repeat calls. Dr. DeWall explained: “A lot of release-of-cares, as we all know, end up utilizing the healthcare system in another way: going to an urgent care, tying up an urgent care or ER bed, or re-utilizing 911 in the near future when they get sicker. We’ve found that this has decreased that return utilization rate as well, so that we're saving time in the long run, not having to go back out and run on those patients a second time.” In the end, said DeWall, there's a significant time savings for time-on-task with telehealth. “Initially, it takes a little more time to learn it and to grease the wheels on the system. But once you get it going, it's very, very efficient.”
While community paramedics can provide patients with a medical analysis and a keen clinical eye that can help address some of their problems, where they really shine is in their ability to help equip patients with the right resources that will truly solve their problems.
McLaughlin said, “EMS was never designed to be the answer for everything. But our healthcare system in America today has gotten so complicated and so difficult that so many times the door is slammed in the face of patients, and they find the ‘wrong door,’ quote unquote, to accessing care. Our approach is: there is no wrong door. We’re the easy button. If you don't know [what to do], reach out to us, and we will help you. We will empower you as the patient to understand what options are available for you and then provide you with contact or resources to get set up with those services.”
In Teller County, community paramedics can help solve problems for patients and connect them with almost any resource they need—whether that’s picking up a prescription or connecting with a behavioral health specialist.
“The goal is to empower you to better navigate this incredibly complicated health care system,” said McLaughlin. “My hope is by the time we part ways, you have a greater understanding of the healthcare system and you have greater healthcare literacy.”
Over the duration of the program, Teller County has seen a significant reduction in costs—by directing patients to the right care from the start. Dr. DeWall shared, “We've been doing a mental health assessment program with Ute Pass Regional Health Service District for about five or six years now, with the goal of decreasing downstream healthcare costs. With our latest calculations, over $4 million of downstream healthcare costs [were] saved by basically being able to divert these patients from an emergency department [and] getting them to a behavioral health crisis center or other community partner.”
Having tangible numbers to show stakeholders has helped continue to secure funding for the program. “For us, it was about having the conversations with the stakeholders,” said McLaughlin. “Who has an interest in sustaining this program? It's the payers, the insurance companies, Medicare, Medicaid.” McLaughlin recommends collecting data and sharing it with stakeholders to help demonstrate the value of the program and how much it saves. “That's why it's so important to collect the data, so that they understand, ‘Hey, this is the money we're saving you.’”
Another way the program helps preserve resources is through team member retention. Dr. DeWall has seen it open up opportunities for longtime members of fire and EMS to continue working.
“[It allows] those providers as they age in fire and EMS to potentially move into a community paramedic role or another role that isn't as taxing on their body, giving them the opportunity to stay in the healthcare continuum for a longer period of time.”
In the midst of a severe staffing shortage, provider satisfaction is another important consideration. By empowering medics with the right tools to get patients the care they need, McLaughlin believes that a telehealth-driven program can help solve some of the factors that lead to burnout.
“Burnout is a byproduct of providers not having the knowledge, skills, abilities, and resources that they need to address the challenges that they've been asked to face. We're ordinary people put in extraordinary situations. And we're not dumb. Paramedics and EMTs are generally really smart. So when you go out there and you see the same patient over and over and over again, and you're not able to get them tied in with the right resources because you don't have the right tools in place to make that happen, that creates frustration. It creates moral injury because you feel like you're contributing to the problem. You want to be part of the solution, and you feel like you should be part of the solution,” said McLaughlin. “This program provides our providers not only with the tools…but also with the additional training and education to be trauma-informed in our approaches and make sure that we're providing services in a manner that don't cause secondary trauma to the patient.”

Throughout the program, the two organizations have kept careful track of data. From fall risk assessments to additional education on how to take prescriptions, the program has helped improve the level of care that patients receive and expand access to care for patients who otherwise would not have received it. According to Dr. DeWall, they were particularly surprised by one of the improvements they saw: patients who are quite sick yet don’t initially want to go to the ER—even when paramedics or EMTs feel their symptoms are severe enough to merit it. As it turns out, telehealth has been able to make the difference in convincing some of those patients that their symptoms are severe enough to seek care at the hospital.
“What they find is that with utilizing telehealth and getting a board-certified ER doctor to say, ‘Hey, listen, this is our concern. This is what we potentially would do for you in the ER,’ we've been able to get about 9% of [those] patients…in the ER ultimately,” said Dr. DeWall. “Of those patients that get referred to the ER and ultimately decide to go when they otherwise would have been a refusal, 64% of those patients ultimately got admitted into the hospital, and 100% of them had some sort of intervention or diagnostic procedure in the ER that otherwise could not be done pre-hospital.”
Making that stat even more impressive is the fact that of the patients that walk in to the ER, 24% are ultimately admitted to the hospital.
“So the fact that 64% of patients who went to the ER after utilizing telehealth and otherwise would have refused care got admitted tells us that we're providing better care and helping these patients, rather than waiting for them to get more sick and utilizing the 911 system in the future,” said Dr. DeWall.
The integrated nature of the telehealth program means that several organizations are collaborating with one another to help treat the same patient. It fosters better, more collaborative relationships between the different organizations and has helped create the feeling of everyone belonging to one cohesive team. According to Dr. DeWall, it’s made a big difference for their teams. “Integrating fire and EMS at all levels of EMS provider, from EMT up through paramedic, critical care paramedic, and community paramedic, has allowed them to interface better by working with emergency medicine physicians and being able to communicate better together, and more effectively.”
The program has also allowed McLaughlin’s team of community paramedics to empower other EMS providers. When other neighboring Basic Life Support transporting agencies are uncertain of what to do, their response is to reach out for mutual aid. “We're not always the answer that the patient needs,” McLaughlin explained. “And so it empowers those agencies to build a stronger partnership with the physician's group and to actually be the answer for the needs in their community. And it allows us to keep our resources in our community and serve our community. It's a win-win for everyone.”

The collaboration also opens up a natural way for responders to learn new things and improve their practice. According to Dr. DeWall, the EMS teams are enjoying the opportunity to pick up new information and insights that can help hone their skills and improve the care they provide. “One thing we hear consistently from our providers who utilize telehealth is that they're actually learning,” said Dr. DeWall. “Each call, they learn more about how the emergency medicine physician is thinking about the patient, different assessment techniques, different questions to ask, that not only helps with the telehealth but helps in their day-to-day care of patients.”
Good partnerships have been an essential component of making the program in Teller County work. McLaughlin credited both UPRHSD’s partnership with Emergency Medical Specialists, the physician group that Dr. DeWall works with, and their joint partnership with Pulsara as important factors in the program’s success.
For those who might be interested in designing a similar program that pairs community paramedics with a group of local physicians, Dr. DeWall believes that the key is in having a partner that is willing to learn and understand both the needs in your community and the resources that are available. “You may not have an emergency medicine group that's close to you or even in-state,” he said. “I think the key is, in-state is helpful. But…more than in-state, you need a physician partner group that is willing to come and learn about your area.”
Acting as a cohesive team is an important part of providing patient care. According to Dr. DeWall, it’s important to have a partner with whom you can have challenging conversations when things aren’t working and work together to formulate solutions. “It [should] seem to the patient, regardless of where the docs are, regardless of those components, that when you're on together, it's you together, working with that patient as a team to develop their care plan collaboratively. That's what I think is the magic in it.”
![]()
To hear James McLaughlin and Dr. Jeremy DeWall share more of the specifics of Teller County’s telehealth initiative, check out the full webinar here: How Fire and EMS Leaders are Turning Telehealth into a Force Multiplier

With record-breaking crowds filling stadiums across North America, the 2026 FIFA World Cup is proving to be one of the largest sporting events in...

June Recap Optimizing Emergency CareLast month, we released our newest feature, Pulsara Intelligence. Built with clinician needs in mind, Pulsara...

In fast-paced clinical settings, manual documentation often competes with vital communication and hands-on patient care. When Pulsara added automated...